I have skim-read the underlying study and read several of the news stories. Basically, my read on it is that this is clickbait crap. The study claims that at the one-drink-per-day consumption level there is a 0.5 percent increase in the RELATIVE risk of developing one of 23 conditions. I.e., it's crap. I have real concerns about the statistical competence of the authors (not exactly a new phenomenon with a disturbingly large share of the medical literature, frankly -- and people talk trash about political science!), and larger concerns about the willingness of the lead author on this study to be quoted in saying ridiculous things like "there is no safe level of consumption" (paraphrasing).
there is no credible evidence in this study of a measurable impact on all-cause mortality OR morbidity of low levels of consumption (1-2 drinks per day) relative to no consumption. And that's without even going to core questions about measurement error.
I am willing to sacrifice my health some to be able to engage in two of my hobbies.
I could be persuaded to give up my wine drinking hobby, but never my beer or whiskey drinking hobbies.
Exactly why it's so important to have a diverse slate of hobbies!
Basically, my read on it is that this is clickbait crap.
Good enough for me. Rack ‘em up!
What I've seen is that the paper is largely right but has been poorly communicated. You touched on that to some extent that the risk increase for moderate consumption is miniscule. Someone else summarized the data as:
According to data provided by the authors but not published in the paper, to suffer one extra alcohol-related health problem, around 1,600 people would need to drink two drinks totaling 20g (2.5 units) of alcohol a day for a year. This is equivalent to around 32 standard 70cl [700 milliliter] bottles of gin over a year, so a total of 50,000 bottles of gin among these 1,600 people is associated with one extra health problem. This indicates a very low level of harm in moderate drinkers and suggests UK guidelines of an average of 16g a day (2 units) are very low-risk indeed.
...
Given the pleasure presumably associated with moderate drinking, claiming there is no ‘safe’ level does not seem an argument for abstention. There is no safe level of driving, but governments do not recommend that people avoid driving. Come to think of it, there is no safe level of living, but nobody would recommend abstention.
I think it is worse than miniscule. I think we really, really, don't know whether there is an increased risk, based on this study, because I lack confidence that they did the math right.
from the paper:
We did a new systematic review for each associated outcome to incorporate new findings on risk and to improve upon existing approaches. This strategy allowed us to systematically control for reference category confounding in constituent studies across associated outcomes. We provide the search strategy, search diagrams, dose–response curves for each included outcome, and references for each outcome in appendix 1 (pp 57–146).
Drawing from our systematic review, we did a meta-analysis of risk outcomes for alcohol use. For each outcome, we estimated the dose–response relative risk curve using mixed-effects logistic regression with non-linear splines for doses between 0 and 12·5 standard drinks daily. We selected 12·5 standard drinks daily as a cutoff point given the absence of available data beyond this range. We present additional details of the model in appendix 1 (pp 51–138). We tested the significance of including a study-level confounding variable on the composition of the reference category (eg, whether former drinkers were included in the abstainer category or not). When found to be significant, this variable was included as a predictor within the model, which was the case for ischaemic heart disease, ischaemic stroke, and diabetes.
Using our dose–response curves, we estimated the consumption level that minimises harm, which is defined in the comparative risk assessment approach as the theoretical minimum risk exposure level (TMREL). We chose a theoretical minimum on the basis of a weighted average relative risk curve across all attributable outcomes. We constructed weights for each risk outcome based on the respective global, age-standardised DALY rate per 100 000 in 2016 for both sexes. Our TMREL was the minimum of this weighted all-attributable outcome dose–response curve.
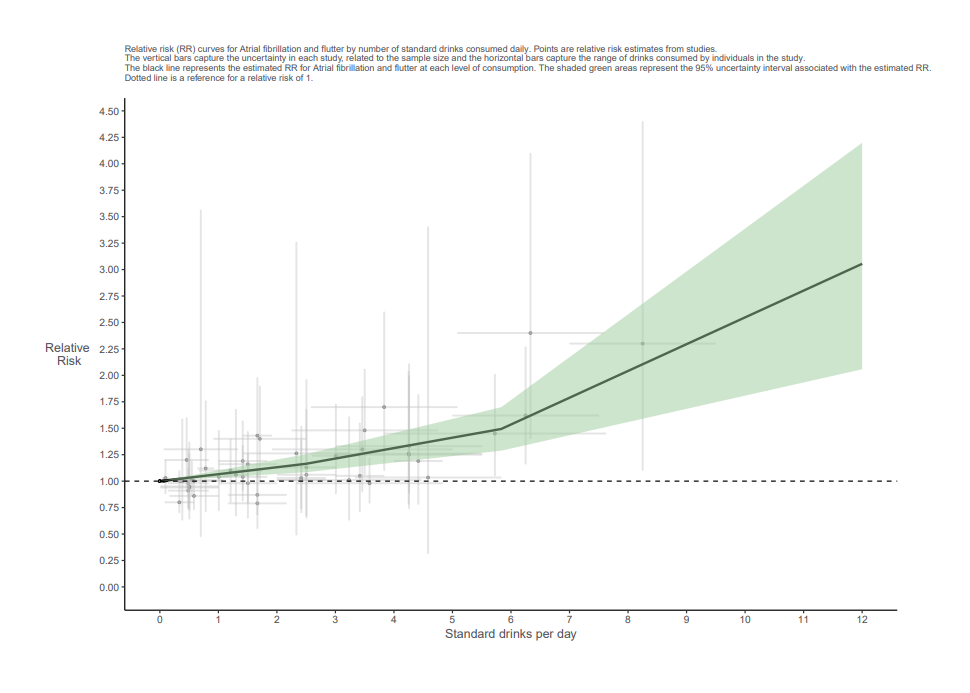
here is the key figure from the article's appendix. It illustrates just one of the 23 outcomes of interest. Note the confidence intervals around the individual data points. Also note the horizontal bars around the individual data points -- indicating the ranges of consumption for individuals in the individual studies. Many of those don't overlap with zero consumption. They are putting a huge burden on the data even in these individual-outcome RR curves.
It also seems likely to me that these types of meta-analysis are very likely to understate systematic bias. The idea is that different studies will have different systematic errors, so combining them helps in the way that having more plate appearances against different pitchers helps us to better judge a hitter, but the systematic errors are surely correlated on some level (similar selection biases across trials, etc) in some way which is more or less unknowable. Even physics, where it is much easier to control things has this issue. If you look at published measurements of the gravitational constant over time, there is a clear confirmation bias at play, where measurements agree really well—for a while—then a new technique comes along and the measurement moves outside the previously-accepted value and all the new measurements are suddenly in good agreement with each other. This even happened in older times when publish or parish was not such an prevalent threat.
As always, even if someone’s methodology is good, I remain skeptical of small effect sizes in any kind of observational study. It is hugely, hugely difficult to reproduce findings in observational studies even under relatively well controlled situations. It’s still good to keep trying and keep improving, but that doesn’t mean I’m going to alter my behavior due to one of these studies.
Ayyup.
"Minor Details" covering Saturday's game is up. We'll have a post covering Sunday's games later this morning, but I have a few things I need to do first.
The first sunspot of Solar Cycle 25 showed up yesterday. Hopefully this one's maximum is more entertaining than the last one was.
This article isn't breaking a lot of new ground but some interesting concepts nonetheless. It appears that the Twins may deploy an Opener every so often in September. What other experiments would you like see tried, during last 5 weeks of a lost season. Definitely strategies to beat the shift could be one.
I'd like them to give a try to winning. And maybe just maybe someone actually hit Joe in when he gets on base.
Winning is old school.
I would definitely like to see the Waxahachie swap more often. With knowledge of player's tendencies, we know which fielder is least likely to be needed on any given batter, so the risk can be minimized and value of platoon pitching maximized. And even if that benefit is marginal, it's a lot of fun.
Official scorers might strike.
Just got home from getting a root canal. Great way to start the week. On Wednesday I’m having surgery for the hernia that the first doctor who saw me three weeks ago said I didn’t have. I seem to be rolling a lot of gutter balls lately.
🚨WE NOW RETURN TO OUR REGULARLY SCHEDULED GAME RESPECTING🚨 Please refrain from using any custom arm sleeves, spikes, bats or personality until next year’s #PlayersWeekend event. Thank you.


Im going to keep trying to prove that study wrong
pfft, small sample size
I have skim-read the underlying study and read several of the news stories. Basically, my read on it is that this is clickbait crap. The study claims that at the one-drink-per-day consumption level there is a 0.5 percent increase in the RELATIVE risk of developing one of 23 conditions. I.e., it's crap. I have real concerns about the statistical competence of the authors (not exactly a new phenomenon with a disturbingly large share of the medical literature, frankly -- and people talk trash about political science!), and larger concerns about the willingness of the lead author on this study to be quoted in saying ridiculous things like "there is no safe level of consumption" (paraphrasing).
there is no credible evidence in this study of a measurable impact on all-cause mortality OR morbidity of low levels of consumption (1-2 drinks per day) relative to no consumption. And that's without even going to core questions about measurement error.
I am willing to sacrifice my health some to be able to engage in two of my hobbies.
I could be persuaded to give up my wine drinking hobby, but never my beer or whiskey drinking hobbies.
Exactly why it's so important to have a diverse slate of hobbies!
Good enough for me. Rack ‘em up!
What I've seen is that the paper is largely right but has been poorly communicated. You touched on that to some extent that the risk increase for moderate consumption is miniscule. Someone else summarized the data as:
I think it is worse than miniscule. I think we really, really, don't know whether there is an increased risk, based on this study, because I lack confidence that they did the math right.
from the paper:
here is the key figure from the article's appendix. It illustrates just one of the 23 outcomes of interest. Note the confidence intervals around the individual data points. Also note the horizontal bars around the individual data points -- indicating the ranges of consumption for individuals in the individual studies. Many of those don't overlap with zero consumption. They are putting a huge burden on the data even in these individual-outcome RR curves.
It also seems likely to me that these types of meta-analysis are very likely to understate systematic bias. The idea is that different studies will have different systematic errors, so combining them helps in the way that having more plate appearances against different pitchers helps us to better judge a hitter, but the systematic errors are surely correlated on some level (similar selection biases across trials, etc) in some way which is more or less unknowable. Even physics, where it is much easier to control things has this issue. If you look at published measurements of the gravitational constant over time, there is a clear confirmation bias at play, where measurements agree really well—for a while—then a new technique comes along and the measurement moves outside the previously-accepted value and all the new measurements are suddenly in good agreement with each other. This even happened in older times when publish or parish was not such an prevalent threat.
As always, even if someone’s methodology is good, I remain skeptical of small effect sizes in any kind of observational study. It is hugely, hugely difficult to reproduce findings in observational studies even under relatively well controlled situations. It’s still good to keep trying and keep improving, but that doesn’t mean I’m going to alter my behavior due to one of these studies.
Ayyup.
"Minor Details" covering Saturday's game is up. We'll have a post covering Sunday's games later this morning, but I have a few things I need to do first.
The first sunspot of Solar Cycle 25 showed up yesterday. Hopefully this one's maximum is more entertaining than the last one was.
This article isn't breaking a lot of new ground but some interesting concepts nonetheless. It appears that the Twins may deploy an Opener every so often in September. What other experiments would you like see tried, during last 5 weeks of a lost season. Definitely strategies to beat the shift could be one.
https://slate.com/culture/2018/08/michael-lorenzen-billy-hamilton-its-time-for-half-the-teams-in-baseball-to-get-weird.html
I'd like them to give a try to winning. And maybe just maybe someone actually hit Joe in when he gets on base.
Winning is old school.
I would definitely like to see the Waxahachie swap more often. With knowledge of player's tendencies, we know which fielder is least likely to be needed on any given batter, so the risk can be minimized and value of platoon pitching maximized. And even if that benefit is marginal, it's a lot of fun.
Official scorers might strike.
Just got home from getting a root canal. Great way to start the week. On Wednesday I’m having surgery for the hernia that the first doctor who saw me three weeks ago said I didn’t have. I seem to be rolling a lot of gutter balls lately.
That guy is great.
This is basically a dream come true for the Emeritus: a story combining LeBron, baseball, and intellectual property law!